 Tiefbiss
mit Bionator, 17-Jährige; Nonokklusion, Scherenbiss
Tiefbiss
mit Bionator, 17-Jährige; Nonokklusion, ScherenbissFunctional treatment of deep bite, 17-yr; non-occlusion
Traitement fonctionnel à 17 ans; dents sans occlusion
Tiefbiss
mit Bionator, 17-Jährige; Nonokklusion, Scherenbiss
Functional
treatment of deep bite, 17-yr; non-occlusion
Traitement
fonctionnel à 17 ans; dents sans occlusion
Funktionskieferorthopädie
(FKO) benötigt Kieferwachstum. Über die
Grenzen dieses Wachstums kenne ich jedoch keine Statistik.
Viele
Ganzheitliche berichten von einzelnen erwachsenen Patienten, bei
denen eine Korrektur der Bisslage mit einem Bionator, Biognathor
(siehe Zahnspangen-Galerie B / Panorama hier
[266kB pdf])
oder anderem FKO-Gerät noch erfolgreich war („Das klappt
nicht immer.“)
Andererseits sind (selten) Rückfälle
der Bissanomalie von Patienten dokumentiert, bei denen diese operativ
korrigiert wurde, ohne die (muskulären) Ursachen zu
beheben.
Denn schließlich baut sich auch erwachsener Knochen
noch auf und ab, und die Lobby für fest eingebaute Apparaturen
zur Bisslagekorrektur baut darauf auf: Herbstscharniere und andere
scharnierartige, flexible oder nach dem Prinzip der
Vorschubdoppelplatte funktionierende Einbauten, die nicht minder
wulstig sind. Ursprünglich zumeist für Spätfälle
gedacht, profilieren sich mittlerweile einige Behandler damit, sie
schon Kindern im Wechselgebiss anzutun! Ihr Haupteinsatzgebiet ist
jedoch das bleibende Gebiss, wo viele Betreiber und Hersteller
Erfolge publik machen.
Logisch folgt daraus aber, dass solche
Spätfall-Erfolge etwas langsamer auch mit herausnehmbaren
FKO-Geräten möglich sein sollten, wenn sie denn konsequent
getragen werden (Biognathor, siehe oben). Zur Retention können
diese Geräte zudem einfach weiterverwendet werden.
Folgende
minimalinvasive Behandlung einer 17-Jährigen, die eine volle
Prämolaren-Breite Unterkiefer-Rücklage bei gutem
Platzangebot hat, stammt aus einer Praxis alter Schule, die nicht als
„ganzheitlich“ gelistet war. Wohingegen mir verschiedene
Fälle bekannt sind, in denen Kieferorthopäden bereits
13-Jährige mit solchen Bissanomalien offenbar als unprofitable
Fälle einstuften und loszuwerden versuchten.
Die
Unterkiefer-Rücklage dieser Patientin ist schon im äußerlichen
Profil erkennbar, samt der bei Tiefbiss typischen „waagerechten“
Unterlippe. Anders als beim rein horizontalen Überbiss (siehe
Fallbeispiel Erwachsenenbehandlung, horizontaler ..), ist der
Lippenschluss beim Tiefbiss, der ein horizontaler und vertikaler
Überbiss ist, nicht erschwert.
Dafür sind Scherenbisse
(Nonokklusionen) dabei häufig: beide Gipfel der oberen
Prämolaren beißen auswärts der unteren Prämolaren.
Diese sind oft in ihrem Wachstum gehemmt, so dass sie unterhalb der
Ebene des Zahnbogens liegen. Ein entsprechend mit „überhängenden
Rampen“ eingeschliffener Aktivator oder Bionator, oder auch
anderes FKO-Gerät wie Fränkel, Bimler oder konfektionierte
Trainer, macht es diesen Zähnen möglich, in ihre korrekten
Positionen weiter zu wachsen. So wird der Scherenbiss und der
vertikale Überbiss simultan mit der horizontalen
Unterkiefer-Rücklage korrigiert. Solche parallelen Korrekturen
sind mit Herbstscharnieren und ähnlich starren Festeinbauten
nicht möglich.
 Nach
2.5 Jahren Bionatorbehandlung ist bei dieser Patientin eine
gesicherte Normalokklusion erreicht. Rechtsseitig erscheinen die
Prämolaren noch etwas kurz, aber ein spontaner Ausgleich ist im
Laufe der Jahre wahrscheinlich.
Nach
2.5 Jahren Bionatorbehandlung ist bei dieser Patientin eine
gesicherte Normalokklusion erreicht. Rechtsseitig erscheinen die
Prämolaren noch etwas kurz, aber ein spontaner Ausgleich ist im
Laufe der Jahre wahrscheinlich.
Zähne und Zahnfleisch haben
unter dieser kostengünstigen Behandlung nicht gelitten, und zur
Retention kann der Bionator einfach ausgeschlichen werden.
Bei
ausgedehntem Scherenbiss (nächste Fotos), der als völlige
Nonokklusion auch Mahlzähne (Molaren) betrifft, kann der
Patient mit kräftigen Seitwärtsbewegungen nur einseitig
kauen. Hier kann ein FKO-Gerät mit zusätzlichen Schlaufen
ausgestattet werden, die sich gegen alle im Scherenbiss stehenden
oberen Zähne richten, wie der rechte Foto-Teil an einem anderen
Patienten zeigt, dessen Eckzähne noch fehlen (wahrscheinlich
beengte Lücken mit Platte vorbehandelt). Zwar wären hier
auch Vorschubdoppelplatten mit oberer Zug- und unterer Dehnschraube
eine Behandlungsoption, aber eine eher nur 2-dimensionale, während
sich Aktivatoren zur 3-dimensionalen Ausheilung auch der vertikalen
Fehlstellungen besser eignen.
Das Gegenteil von Scherenbiss,
der Backenzahn-Kreuzbiss, bestand im letzten Foto isoliert an
einem 6er. Auch für seine Korrektur parallel zur allgemeinen 3-D
Bisslagekorrektur kann ein Aktivator oder Bionator ausgerüstet
werden, wie hier gezeigt: den unteren Kreuzbiss-Zahn einwärts
und den oberen auswärts lenken. Dennoch habe ich schon einen
Fall nach vollständiger kieferorthopädischer Behandlung im
Jugendalter gesehen, bei dem ein 6er-Kreuzbiss von der Behandlung
ausgespart worden war.
 Functional
orofacial orthopedics requires
jaw growth. I don´t have statistical data about the limits of
this.
Functional
orofacial orthopedics requires
jaw growth. I don´t have statistical data about the limits of
this.
Many holistic dentists report cases of
adult patients, where overbite still was healed by means of removable
functional appliances (see Gentle braces B chapter; in Germany,
mainly bionators here).
However,
this does not work in any adult case.
On the
other hand, relapses occur (rarely) even at patients whose overbite
or other malocclusion had been corrected by bone surgery – when
no attention had been paid to muscular disorders which can cause
malocclusions.
In
adult bone, processes of growth and
decomposition still take place, and the lobbies
of „fixed functional orthopedics“ (FFO) argue by this. Such
inconvenient appliances were mainly intended for teenage and adult
patients, but certain orthodontists try them even on children in
mixed dentition. But most
of the published cases started in permanent
dentition. This leads to the conclusion that appropriate removable
appliances should also succeed in late cases, however slower and only
if worn sufficiently, of course. Comfort is crucial, and the last
appliance in use
can serve as a retainer then, by simply reducing
its daily wearing time.
The
case presented here is a minimal invasive treatment of a 17-yr lady,
whose lower jaw was lying back by a full bicuspid width, with plenty
of space. The doctor who offered this treatment practised the former
common European style, but was not in a list of holistic dentists. In
contrast, I know cases in which „modern“ orthodontists
wanted to get rid of just 13-yr old patients who had the same
malocclusion, but maybe appeared to them as not profitable
enough.
The backward position of the patient´s lower jaw can
already be seen from her chin. Viewed from the side, the lower lip
appears horizontal, as typical for a deep bite. Lip seal is not
hampered, in contrast to cases which bear a large overjet without
increased overbite (for this, see case chapter: Adult treatment of
horizontal ..).
Deep bite is frequently accompanied by
non-occlusion of bicuspids: both summits of the upper stand outside
the lower bicuspids. These are often impeded in their vertical
development, so that they are below the level of the incisors and
molar teeth. If an activator or bionator is carved according to this
with „hanging ramps“, these teeth can resume their
development and can be directed to their correct positions while they
grow. This works also with other functional appliances, as those of
Fränkel or Bimler, or (see that case chapter) prefabricated
trainers. Overall, non-occlusion, vertical overbite and horizontal
overjet are treated simultaneously, what is impossible to this extent
by Herbst and other rigid fixed appliances.
After 2.5
years of bionator treatment,
the presented patient has reached a normal occlusion. On her right
side, the bicuspids are still somehow short, but this will probably
equilibrate within the next years. Teeth and gums have not suffered
from this economic treatment, and for retention, the daily wearing
time can be continuously reduced.
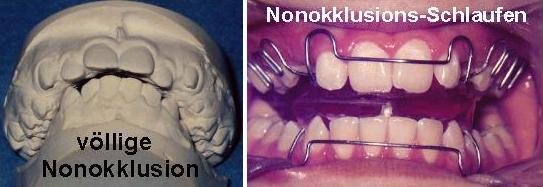 In
case of general non-occlusion, which even includes molar teeth
(next images), the patient can never chew on both sides at once. An
appropriate functional appliance for this can be equipped with
additional lateral loop springs, which are directed against any
non-occluding upper tooth. This is shown in the right part of the
image from another patient, who is still lacking his cuspids
(perhaps, space for them was just re-gained by a
segmented plate appliance). Another way to treat this would be
bite-jumper plates (or twin
blocks) with a traction screw in the upper and an expansion screw in
the lower part. But this combination would rather act
in 2 dimensions, whereas 1-piece functionals
are superior to heal deviations also
in the third, vertical dimension.
In
case of general non-occlusion, which even includes molar teeth
(next images), the patient can never chew on both sides at once. An
appropriate functional appliance for this can be equipped with
additional lateral loop springs, which are directed against any
non-occluding upper tooth. This is shown in the right part of the
image from another patient, who is still lacking his cuspids
(perhaps, space for them was just re-gained by a
segmented plate appliance). Another way to treat this would be
bite-jumper plates (or twin
blocks) with a traction screw in the upper and an expansion screw in
the lower part. But this combination would rather act
in 2 dimensions, whereas 1-piece functionals
are superior to heal deviations also
in the third, vertical dimension.
The
opposite of non-occlusion, the lateral crossbite, affected a
single molar tooth in the last image. It is shown how a functional
appliance can be equipped to correct this in parallel to the general
3-dimensional orthopedic treatment: appropriate springs direct the
lower molar inward, and its counterpart outward. Nevertheless I once
met a man who had a full orthodontic treatment as a teenager, but
still a single molar crossbite which had not been treated there.
L´orthopédie
dento-faciale fonctionnelle
nécessite de la croissance maxillaire. Il me manque de la
statistique sur les facteurs limitants ici.
En tout cas, nombreux
dentistes holistiques rapportent des cas cliniques de
décalage (classe II), qui étaient guéris même
en âge adulte par les appareils amovibles. Au section Appareils
doux B (fonctionnelles), ces sont en Allemagne surtout les
bionateurs, mais en France plutôt les
activateurs souples préfabriqués. Néanmoins, ils
ne marchent pas toujours chez
l´adulte.
D´autre part, des récidives se
sont manifestées même aprés de la chirurgie
maxillo-faciale – si les influences musculaires qui peuvent
causer la malocclusion étaient été
négligés.
L´os adulte se forme et se décompose
toujours, et le lobby des soi-dites appareillages fonctionnelles
fixes en tire profit. Ces appareils gênants sont surtout conçus
pour les ados et adultes, mais néanmoins il y a des
orthodontistes qui les essaient même aux enfants aussi jeunes
que 8 à 11 ans! Mais le plupart des cas publiés ont
subi ce traitement en dentition permanente. Par logique, l´orthopédie
fonctionnelle tardive
devrait aussi marcher en appareillage amovible, cependant moins vite
et sous condition que l´appareil sérait porté
suffisamment. Son confort est essentiel, et le dernier appareil peut
ensuite servir pour la contention, en réduisant simplement le
temps de port quotidien.
 Le
cas clinique présenté ici est une patiente de 17 ans
qui était traitée de façon minimal-invasive.
Sa mâchoire inférieure était en arrière
par une distance d´une entière prémolaire (classe
II molaire complète). Toutefois les dents ont assez d´espace.
Le dentiste spécialisé qui donnait ce traitement le
faisait en ce système qui était jadis très
répandu en Europe. Il ne figurait pas dans une liste des
holistiques. Au contraire, quelques médiocres orthodontistes
„modernes“ rejetent des patients d´une telle
malocclusion même s´ils sont aussi jeunes que 13 ans.
Peut-être ils les jugent comme peu profitables.
Le
cas clinique présenté ici est une patiente de 17 ans
qui était traitée de façon minimal-invasive.
Sa mâchoire inférieure était en arrière
par une distance d´une entière prémolaire (classe
II molaire complète). Toutefois les dents ont assez d´espace.
Le dentiste spécialisé qui donnait ce traitement le
faisait en ce système qui était jadis très
répandu en Europe. Il ne figurait pas dans une liste des
holistiques. Au contraire, quelques médiocres orthodontistes
„modernes“ rejetent des patients d´une telle
malocclusion même s´ils sont aussi jeunes que 13 ans.
Peut-être ils les jugent comme peu profitables.
La classe II
de cette patiente se voit déjà à son menton.
Regardé par le côté, sa lèvre inférieure
est horizontale, ce qui est typique pour le décalage profond.
La fermeture de la bouche est sans problème, au contraire aux
cas dont le décalage est surtout horizontal (y trouvez un cas
au chapitre Traitement de classe II (horizontale) chez l´adulte).
Le
décalage profond est souvent accompagné par les
prémolaires hors d´occlusion: tous les deux sommets des
prémolaires supérieures sont à l´extérieur
des prémolaires inférieures. Celles-ci sont souvent
sous-développées en direction verticale, et paraîssent
en dessous du niveau des incisives et molaires. Un activateur ou
bionateur peut être rodé en telle façon que ces
dents peuvent reprendre leur éruption. En cette voie, elles
peuvent être dirigées au long des rodages vers leurs
positions saines. Cette croissance controlée marche aussi avec
des autres appareils fonctionnels, comme ceux de Fränkel, de
Bimler ou des activateurs préfabriques de type Soulet-Besombes
(voir le chapitre sur l´ODF neuro-musculaire avec ..
préfabriqués). Dents en fausse occlusion, décalages
horizontaux et verticaux peuvent être guéris en même
temps, ce qui n´est pas possible avec des bielles de Herbst ou
autres appareillages fixes rigides.
Après 2.5 années
de bionateur, la patiente à achevé l´occlusion
normale. Au côté droit, ses prémolaires
paraîssent toujours un peu trop courtes, mais probablement
continueront leur évolution lentement. Les dents et gencives
n´ont pas souffert sous ce traitement, qui est en plus peu
coûteux. Ensuite, le temps de port quotidien sera réduit
pour la contention.
En
cas de non-occlusion globale, qui comprend même les
molaires (photo suivante), une mastication normale, bilatérale
n´est pas possible. Un appareil fonctionnel approprié
peut être équipé en ce cas avec des élements
latéraux supplémentaires, qui sont réglables
contre chaque dent supérieure qui est hors d´occlusion,
comme montré au droite. Cette photo vient d´un autre
patient, qui manque toujours ses canines. Peut-être, leur
espace à justement été re-gagné par une
plaque à vérins. Des Plaques-propulseurs, y inclu le
PUL, séraient une autre méthode aptée ici, si
munis d´un vérin d´expansion à l´inférieure
et d´un vérin de traction à la supérieure.
Mais cet ensemble agira plutôt en 2 dimensions, pendant que les
appareils en une pièce sont meilleurs pour guérir aussi
les malocclusions verticales, à dire la 3ème
dimension.
Le contraire à la non-occlusion, l´articulé
inversé latéral, a atteint seulement une molaire à
la dernière photo. L´activateur montré est équipé
pour le corriger en même temps avec le traitement orthopédique
générale des mâchoires. Une paire des ressorts
dirigera la molaire inférieure vers l´intérieur
et son pendant vers l´extérieur. Cependant, j´ai
connu un homme qui a subi un traitement orthodontique complet quand
il était jeune, mais avait toujours un articulé inversé
d´une molaire qui n´y avait pas été traité.
Quellen
sources: Dr. Hermann Voß,
44229 Dortmund, Tel. 0231 730651
zurück
back retour
Letztes
Update dieses Teils +++ last
update +++ dernière
mise à jour: 11.05.2009