Lücken-Rückgewinnung,
im Wechselgebiss und präprothetisch
Lücken-Rückgewinnung,
im Wechselgebiss und präprothetischRecovery of gaps, in mixed dentition and pre-prosthetic treatment
Rétablissement des lacunes, en dentition mixte et traitement pre-prothétique
Lücken-Rückgewinnung,
im Wechselgebiss und präprothetisch
Recovery
of gaps, in mixed dentition and pre-prosthetic
treatment
Rétablissement
des lacunes, en dentition mixte et traitement pre-prothétique
Platz für Zähne
kann durch generellen Platzmangel im Kiefer fehlen, wie hier im 1.
Beispiel, oder durch kontraproduktive Zahnwanderung wie in den
weiteren Beispielen.
Die folgenden 6 Beispiele von Behandlungen
mit aktiven Platten sind nach
fortschreitendem Zahnwechsel geordnet. Gut konstruierte
Platten bei gut mitarbeitenden Patienten sichern jedoch noch keinen
Erfolg, sondern es kommt auch auf sorgfältige
Behandlungsführung an. Die Platten sind für
Zahnbewegungen und nachwachsende Zähne
gezielt auszuschleifen, es darf nicht schneller geschraubt werden,
als das individuelle Wachstum mitkommt, und vor allem sollten Platten
stets guten Halt haben. Dieser kann sich beim Weiterschrauben
nämlich verschlechtern, und sorgfältiges Nachstellen
kann dann bis zu 15 Minuten beanspruchen.
Beispiel
1:
Sohn
einer Zahnarzthelferin, rechtzeitig
mit noch 12 Milchzähnen begonnene
Behandlung, ähnelt dem Fall aus älterer
Quelle, der in Engstand:
Zähneziehen vermeiden mit Details der
Platten beschrieben ist.
 Zahn-Engstand
ist eine Zivilisationskrankheit,
und das Risiko dafür kann verringert werden, indem man Kindern
frühzeitig reichlich kauintensive Nahrung statt Weichkost gibt,
aber ein Garant gegen Endstand ist dies nicht. Z.B. haben von
Geschwistern, die die gleiche ländliche Kost bekamen, einige
Engstände entwickelt, und andere nicht.
Zahn-Engstand
ist eine Zivilisationskrankheit,
und das Risiko dafür kann verringert werden, indem man Kindern
frühzeitig reichlich kauintensive Nahrung statt Weichkost gibt,
aber ein Garant gegen Endstand ist dies nicht. Z.B. haben von
Geschwistern, die die gleiche ländliche Kost bekamen, einige
Engstände entwickelt, und andere nicht.
Ein
ausgeprägter Engstand der neu wachsenden Schneidezähne wie
hier ist schon vorher daran absehbar, dass die Milch-Schneidezähne
nicht auf Lücke gehen. Für so frühe Behandlung bieten
sich kostengünstige konfektionierte Trainer an, siehe
Unterkapitel Neuromuskuläre
Behandlung.
Das erste Mundfoto und
Gipsmodell erfolgten noch vor Behandlungsbeginn und zeigen im
Oberkiefer beengte Lücken für die 2er und schiefe 1er.
Unten drängen sich 4 wachsende Schneidezähne, wo nur Platz
für 3 ist, und Kopfbisse drohen.
Das 1. Platten-Paar enthält
Bertoni-Schrauben oben und unten, und eine Fingerfeder gibt dem
auswärts ragenden 1er Druck zur Mitte. Wachsende unteren
Schneidezähne entfalten sich bei Platzgewinn in diesem Stadium
oft noch selbst in die Reihe. Das untere
Gipsmodell zeigt eine gute Platz-Situation nach 4.5 Jahren, mit
gerader UK-Front und oben tadellos parallelen 1ern, während die
2er noch eine Restkorrektur brauchen. Diese wachstumsbegleitende
Behandlung ist noch nicht ganz abgeschlossen,
da noch 2 Milch-5er vorhanden sind, aber wenn nur noch geringe
Korrekturen anstehen, kann die tägliche Tragezeit reduziert
werden. Dann erscheint der Aufwand an Zeit durch die
Dauer dieser Behandlung geringer, die ohne belastende oder
kostenintensive Behandlungsmittel auskam.
Individuelle Unterschiede in der Zahnbeweglichkeit und in der Dauer der Zahnwechselphase (dentitio tarda = zögerlicher Zahnwechsel) wirken sich auf Platten-Behandlungen aus. Wobei auch für die Langzeitstabilität nach kieferorthopädischen Behandlungen gilt: Gut Ding will Weile haben.
|
Beispiel 2: oben noch 4 Milchzähne,
Engstand mit Pflugscharstellung der 1er und Kreuzbiss eines 2ers,
unten noch 5 Milchzähne und Totalverlust des Platzes für
einen Eckzahn: der etwas einwärts stehende 2er links im Bild
grenzt an den Milch-4er. |
 |
 |
Beispiel
3: Noch je 3 Milchzähne oben und
unten, unterer Zahnbogen gesund, aber schmaler Oberkiefer mit
Totalverlust einer 5er-Lücke! Offenbar war hier der Milch-5er
zerstört und vorzeitig entfernt worden, und der 6er ist bündig
aufgerückt. 3 Zähne brauchen dort Platz, wo jetzt ein
Milch-3er und -4er stehen. Auf der Gegenseite, wo die Prämolaren
schon gewechselt sind, hat der Zahnbogenverlauf eine Delle, die von
einer (leichten) Einengung herrühren kann.
Da dieser Patient
offenbar eine höhere Zahnbeweglichkeit hatte als die anderen
hier gezeigten, und einen schnelleren Zahnwechsel, war nach nur 1 3/4
Jahren nicht nur der aufgewanderte 6er um 7 mm distalisiert,
sondern auch die Zähne davor eingeordnet, die Zahnbögen
ausgeformt, der Oberkiefer 9 mm verbreitert und der
Unterkiefer angeglichen. Zur abschließenden Feinarbeit an den
Eckzähnen hätte der Patient zwar noch Lust gehabt, aber der
Zahnarzt nicht mehr.
 Beispiel
4: 2 beengter
Eckzahn im Unterkiefer, oben noch 2 Milchzähne, Eckzahn-Lücke
links im Bild um 4mm verengt, Schneidezähne
übergewandert, hingegen wirkt der 6er hier nicht
aufgewandert. Hier hat vermutlich der 4er den Milch-3er mit
ausgetrieben und ist dann vor Platz-Überschuss gedreht in beide
Lücken gewachsen. So zeigt die seitliche Ansicht Kopfbisse
im Prämolarenbereich.
Beispiel
4: 2 beengter
Eckzahn im Unterkiefer, oben noch 2 Milchzähne, Eckzahn-Lücke
links im Bild um 4mm verengt, Schneidezähne
übergewandert, hingegen wirkt der 6er hier nicht
aufgewandert. Hier hat vermutlich der 4er den Milch-3er mit
ausgetrieben und ist dann vor Platz-Überschuss gedreht in beide
Lücken gewachsen. So zeigt die seitliche Ansicht Kopfbisse
im Prämolarenbereich.
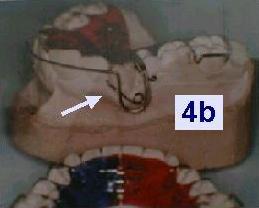
Etwa 4
Jahre Behandlung bis zu den wohlgeformten, symmetrischen Zahnbögen
mit Normalokklusion in den Abschlussmodellen. Die Platten im
Behandlungsverlauf eines ähnlichen Falles 4b
ordnen einen vorstehend wachsenden Eckzahn mit einer Rückholfeder
ein.
Platte
Beispiel 5:
jugendlich, frisches bleibendes Gebiss, Eckzähne vor Enge in
diesem Fall nicht vorstehend, sondern verdreht. Diese Platte enthält
neben einer 3-Wege-Schraube, die den Eckzahnbereich erweitert, noch 2
Distalschrauben, so dass sie 5-gliedrig ist. Diese
Zusatzsegmentierung hilft, Gegenkräfte aufzuteilen und einen
übermäßigen Vorschub der Schneidezähne so zu
vermeiden. Da die 7er bei Jugendlichen zur Distalisierung schlecht zu
greifen sind, ist diese über die 6er zu stemmen.
Anders als
Sparversionen ist diese
Platte zudem als Vollversion darauf ausgelegt, die Eckzähne im
Zuge des Platzgewinns auch gleich zu derotieren.
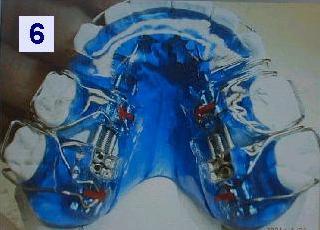
Platte
Beispiel 6: ältere Patientin,
präprothetische Behandlung, alle 4
Prämolaren fehlen:
2 wurden schon in der Jugend gedankenloser
Kieferorthopädie geopfert, und 2
waren später zerstört. Für diese steht Zahnersatz an,
aber die Mahlzähne sind schon vorgewandert und haben die Lücken
eingeengt. Zur Lücken-Rückgewinnung hat diese Platte
ein Paar spezielle Doppeldistalschrauben mit
je 2 unabhängigen Segmenten („reziproke Zug-
und Druckschraube“; zum Nachmachen mit Standard-Schrauben, siehe
Zahnspangen-Galerie A). Dabei sind
die 7er im diesem älteren Gebiss
besser zu ergreifen als im jugendlichen.
 |
|
Space
for teeth can lack due to a general shortage of space in the jaw, as
in the 1. example here, or due to space-consuming forward migration
of teeth, as in the other examples.
6 examples of treatments
with plate appliances follow in sequence of progressive age of
their dentition. Well-designed plates and cooperative patients do not
yet secure a success, however, but the appliances also need to be
carefully adjusted in each control session. The target positions
for growing or moved teeth in the plate have to be ground free, and
screws must not be cranked more often than the individual jaw growth
or tilt-free tooth mobility can catch up. Moreover, plates should
always snap in firmly. A good fit can deteriorate when plates are
screwed, and then, a proper re-adjustment may take up to 15 minutes.
Patient
1: son of a dentist´s assistant, treatment started well in
time with still 12 milk teeth left. This case resembles that from
older sources in Crowding
:avoid extractions,
where the appliances are described more in detail.
Crowding
teeth are a civilisation disease. The risk for it can be lowered
by feeding children early with hard food, but in cannot be brought to
zero. Of siblings who grew up with the same rural cooking, e.g., some
developped straight teeth and others crowded.
Such
a pronounced crowding of growing incisors can be expected even
earlier, and treated e.g. with inexpensive prefabricated trainers
(see subchapter Myofunctional
treatment), namely if
no gaps appear between the milk teeth before they fall.
The first
mouth photo and plaster models were taken before treatment started.
In the upper jaw, they show narrowed gaps for the lateral incisors
and crooked central incisors. Below, 4 growing incisors crowd in a
space for 3, and are in danger to bite summit-on-summit.
The first
upper and lower plates both contain a 3-way expander (Bertoni screw),
and a wire finger directs the outstanding incisor into the row.
Crowded lower incisors which still grow, as here, often unfold
themselves in a proper row if sufficient jaw growth is stimulated.
The lower plaster models show straight lower incisors and upper
central incisors after 4.5 years, whereas the upper side incisors can
be further aligned, since with still 2 milk molars left, treatment is
not yet finished. Nevertheless, the daily wearing time can be
reduced. This alleviates the duration of this not speedy, but
low-risk, inexpensive and formerly well-proven method.
Individual
differences exist as well in tooth mobility as in the duration of
the phase of mixed dentition, and those affect the duration of these
treatments. Long-term stability is often better after slow than after
rapid aligning.
Patient 2: in the upper jaw still 4 milk
teeth, crowded incisors with a single crossbite, in the lower jaw 5
milk teeth and a total loss of the gap for the cuspid which is to
come on the left side in the photo, where a slightly inward-bent
incisor is adjacent to a milk molar. Teeth which grow slightly off
within the dental arch can make 2 milk teeth fall out. This
may have caused the premature loss of the milk cuspid here, and then,
the gap closed from both sides.
The plaster casts in the middle
show well aligned arches in the fresh permanent dentition.
Vertically, however, the lateral front teeth are not yet fully
developped. The not-narrowed lower canine tooth seemed to have
erupted outside the row and to have been aligned.
The last plaster
casts were taken after 1 year in retention. They show a healthy
occlusion of well-aligned teeth.
 Patient
3: still 3 milk teeth in each jaw, lower arch healthy, but narrow
upper jaw with a total loss of the 5 gap. Obviously the milk-5 had
been pulled prematurely, and the firct permanent molar (6) moved up.
3 teeth will need space there where now milk-3 and milk-4 are. On the
opposite side, all teeth except the cuspid have already changed, and
the arch has a dent which could stem from a slight narrowing. This
patient had a higher tooth mobility and completed his permanent
dentition faster than the other examples here, so that in the second
plaster cast after only 1 3/4 years, not only the advanced molar had
been distalized by 7 mm, but also the new teeth were aligned,
the arch shaped well and expanded by 9 mm, and the lower arch
adjusted to this. The alignment of the cuspids could still be
improved, and the patient was willing to this, but the dentist was
uninterested to continue.
Patient
3: still 3 milk teeth in each jaw, lower arch healthy, but narrow
upper jaw with a total loss of the 5 gap. Obviously the milk-5 had
been pulled prematurely, and the firct permanent molar (6) moved up.
3 teeth will need space there where now milk-3 and milk-4 are. On the
opposite side, all teeth except the cuspid have already changed, and
the arch has a dent which could stem from a slight narrowing. This
patient had a higher tooth mobility and completed his permanent
dentition faster than the other examples here, so that in the second
plaster cast after only 1 3/4 years, not only the advanced molar had
been distalized by 7 mm, but also the new teeth were aligned,
the arch shaped well and expanded by 9 mm, and the lower arch
adjusted to this. The alignment of the cuspids could still be
improved, and the patient was willing to this, but the dentist was
uninterested to continue.
Patient
4: narrowed cuspid below, still 2 milk molars in the upper jaw.
The gap for the upper cuspid in the left side of the photo is
narrowed by 4 mm, and the incisors have migrated over, whereas the 6
stayed in place. It seems here that the growing 4 expelled also the
milk-3 (cuspid) and then grew slightly rotated in the middle of both.
The lateral view reveals the top-on-top bite of these premolars.
It
took approximately 4 years until the well-shaped, properly aligned
symmetrical arches and normal occlusion in the final plaster casts.
The plates in the course of the treatment of a similar case 4b
show a particular element, the retractor spring, which directs a
cuspid that grows outside the row and too frontal, as it frequently
happens, into the gap which already had been opened sufficiently.
Plate
example 5 for a teenager with fresh permanent dentition:
narrowing of cuspids caused them here not to stick out, but to grow
rotated. Therefore, this plate contains a 3-way-expander for
broadening the cuspid region, and moreover, 2 screws for molar
distalization. So it has 5 segments in total, and the distal
segmentation serves to distribute the counter-forces more evenly, so
that an exaggerated protrusion of the incisors can be prevented.
Since the 7s of teenagers are difficult to grab firmly with clasps,
they are to be pushed back by the 6s which are better to grab. Unlike
primitive plate appliances which serve just to prepare a fixed
treatment, this one is outlayed for full treatment, as can be
presumed from the additional wire loops which are to derotate the
cuspids already during their space is recovered.
Plate example
6 is for pre-prosthetic treatment of an elderly patient, where
all 4 premolars are missing: 2 had been sacrified to thoughtless
orthodontics in the youth, and 2 were destroyed later. They are to be
replaced now, but a migration of the molars has already narrowed
their gaps too much. To recover them, this plate is equipped with a
pair of special, double distal screws which bear 2 independent
segments each („traction and compression screw“, see in the
Gentle braces A chapter how to imitate it with standard screws). Here
in the elderly dentition, the 7s are better to grab than in the young
example above.
 L´espace
pour les dents peut manquer à cause d´un défaut
du développement maxillaire, comme au premier cas ici, ou à
cause d´un avancement des certaines dents, comme dans les
autres cas.
L´espace
pour les dents peut manquer à cause d´un défaut
du développement maxillaire, comme au premier cas ici, ou à
cause d´un avancement des certaines dents, comme dans les
autres cas.
6 cas cliniques des traitements en plaques mobiles
sont au suivant classés par ordre de leur âge dentaire.
Les plaques bien contruites et les patients coopératifs
n´assurent pas encore le succès, cependant, mais il faut
aussi régler les appareils soigneusement à
chaque rendez-vous de contrôle. Les positions de destination
pour les dents sont à roder, soit qu´elles poussent
ou soit qu´elles sont à déplacer. Les
vérins ne doivent pas être tournés plus
fréquemment que la croissance individuelle peut suivre, ou que
les dents peuvent être déplacées sans qu´elles
s´inclineraient. Il faut en plus que les plaques s´enclenchent
toujours bien. Quand on utilise des vérins, les plaques qui
étaient bien adaptées au debut commencent parfois à
vaciller. La re-adaptation soigneuse peut alors prendre jusqu´à
15 minutes.
Cas
clinique 1: fils d´une assistante dentaire, avec toujours
12 dents de lait. Le traitement était commencé en temps
utile. Ce cas est semblable à celui-là d´une plus
vieille source dans EVITER
DES EXTRACTIONS, où les appareils sont
décrits en détail.
Les dents bousculantes sont
une maladie de civilisation. On peut baisser son risque par
donner aux enfants de la nourriture dure dès le plus jeune
âge, mais on ne peut pas l´exclure. Parmi quelques soeurs
qui grandissaient avec le même régime champêtre,
par exemple, les unes
déployaient des dents bien alignées, et les
autres des dents chevauchantes.
On peut déjà
escompter un encombrement des neuves incisives si les lactéales
ne s´espacent pas avant qu´elles tomberaient. Pour
traiter les encombrements en voie de développement, les
activateurs souples pre-fabriqués
séraient un moyen doux et économique (voir au
sous-chapitre ODF
neuro-musculaire).
La
première photo orale et modèle en plâtre étaient
prises avant le debut du traitement. À la mâchoire
supérieure, les lacunes pour les incisives latérales
sont rétrécies et les incisives centrales sont de
travers. En bas, 4 incisives bousculent là où l´espace
ne suffirait que pour 3, et risquent de mordre bout-à-bout.
Toutes
les deux plaques premières contiennent des écarteurs à
3 directions (vérin de Bertoni), et un doigt en fil de fer
dirige l´incisive saillante vers l´arcade. Incisives
chevauchantes inférieures qui poussent toujours, comme ici, se
déployent souvent toutes seules quand la croissance maxillaire
sérait stimulée. Les modèles suivants montrent
que ces incisives de bas et aussi les incisives centrales au
supérieur sont bien alignées, après 4.5 années.
L´alignement des incisives latérales de haut peut
toujours être affiné, mais la dentition est toujours
mixte avec 2 molaires lactéales, et ainsi le traitement n´est
pas encore terminé. Cependant, le temps de port quotidien peut
être réduit, ce qui allégerait la durée de
cette méthode qui n´est pas rapide, mais peu coûteuse,
peu dangereuse et bien épreuvée jadis.
Des
différences individuelles existent à la mobilité
dentaire aussi qu´à la durée de la phase de
dentition mixte. Elles se répercutent sur la durée du
traitement, et la stabilité á long terme est en général
supérieure après l´ODF lente qu´après
une orthodontie rapide.
Cas
clinique 2: à la mâchoire supérieure, 4 dents
de lait, étroitesse pour les incisives avec un articulé
inversé isolé. À la mâchoire inférieure,
5 dents de lait et perte totale de la lacune pour la canine au gauche
de la photo. Là, l´incisive latérale est inclinée
un peu vers l´intérieur et est attenant de la molaire de
lait. Dents qui poussent dans l´arcade un peu hors position
peuvent faire tomber 2 dents de lait, ce qui semble d´avoir
enlevé la canine lactéale ici. Puis, sa lacune s´était
fermée des deux côtés.
Les deuxièmes
modèles en plâtre arborent des arcades bien alignées
à la neuve dentition permanente. En vertical, cependant, les
incisives latérales et les canines n´ont pas encore
terminé leur développement. La canine inférieure
qui n´était pas mise à l´étroit
semble d´être poussée saillante et était
alignée. Les derniers modèles étaient prises
après 1 année de contention. Ils montrent des belles
arcades en occlusion normale.
Cas clinique 3: toujours 3 dents de lait à chaque mâchoire, l´arcade inférieure est saine, mais la supérieure est étroite et a complètement perdu la lacune d´une 5. Apparemment, la molaire de lait y avait été enlevé précocement, et puis, la molaire permanente (6) avançait jusqu`au contact. 3 dents auraient besoin d´espace là où se trouvent actuellement la 3 et la 4 lactéale. À l´autre côté, seulement la canine est toujours lactéale, et l´arcade est fléchi vers l´intérieur, probablement à cause d´un léger rétrécissement. Comparé aux autres cas, la mobilité dentaire de ce patient était supérieur. En plus, il a achevé sa dentition permanente plus vite, et ainsi, les derniers modèles montrent après seulement 1 3/4 années que la molaire avancée était re-distalisée par 7 mm, et en même temps, toutes les autres dents étaient rangées, avec une expansion de l´arcade supérieure par 9 mm, et l´arcade inférieure y ajustée. L´alignement des canines pourrait toujours être affiné, et le patient était de bonne volonté, mais le dentiste n´y était plus intéressé.
Cas
clinique 4: canine à l´étroit en bas,
toujours 2 molaires de lait en haut, et la lacune pour la canine au
gauche de la photo rétrécie par 4mm. Les incisives
étaient traversées vers la lacune, pendant que la
molaire permanente n´avait pas bougé ici. Apparemment,
la prémolaire (4) a fait tomber aussi la canine de lait et
puis, elle est poussée, quelque part pivotée, au milieu
des deux lacunes. La vue de côté révéle
que les prémolaires mordrent bout-à-bout.
Ce
traitement a mis 4 années environ jusqu´aux arcades
symétriques et bien alignées et l´occlusion
normale que les deuxièmes modèles montrent. Pour un cas
4b qui est similaire, la plaque supérieure de suite est
muni d´un élément particulier, un ressort
rétracteur. Ceci sert à diriger cette canine vers
d´arcade, qui pousse hors de l´arcade et avancée,
comme chez pas mal des enfants. Sa lacune avait déjà
été assez élargi.
La
plaque d´exemple 5 est pour un adolescent en dentition
permanente fraîche. Ici, l´étroitesse n´a
pas déplacé les canines vers l´extérieur,
mais les a fait pivoter. Alors cette plaque contient un écarteur
à 3 directions (vérin de Bertoni) pour élargir
ces régions, et en plus, 2 vérins latéraux pour
la distalisation des molaires, ce qui fait au total 5 segments. Les
segments distaux servent à distribuer la contre-force et
peuvent ainsi éviter que la vérin de Bertoni avancerait
les incisives trop. Car les molaires 7 des adolescents sont
difficiles à saisir par les crochets, elles sont à
repousser par les molaires 6 qui sont plus facile à saisir. À
l´opposé des plaques primitives qui préparent
seulement un traitement en fixe, cette plaque est construite comme un
moyen de traitement autonome. Les éléments pour
l´alignement ne manquent pas, en ce cas des pliages additifs
contre les canines, pour les faire déroter aussitôt que
l´espace pour elles sérait libéré.
La
plaque d´exemple 6 est pour le traitement d´une
patiente plus âgée, à laquelle manquent toutes
les 4 prémolaires: 2 avaient été sacrifiés
à l´orthodontie irréfléchie á
l´adolescence, et 2 étaient détruites plus tard.
Celles-ci sont à remplacer maintenant, mais l´avancement
des molaires a déjà rétréci les lacunes
trop. Afin de les regagner, cette plaque est equipée d´une
paire des vérins doubles qui portent 2 segments indépendants
chacun. Trouvez au chapitre Appareils doux A comment on peut imiter
cet élément spécial avec des vérins
standard. Ici dans la dentition âgée, les molaires 7
sont plus faciles à saisir qu´à la dentition
jeune de ci-dessus.
Quellen sources: Beispiel 1: Praxis R. Lockenvitz, D - 57627 Hachenburg; Technik bei allen 6 Beispielen: www.kfo-soehngen.de (auch Unterstützung bei Behandlungsplänen, Beratung von Patienten und Zahnärzten, Lehrgänge für Zahntechniker und Zahnärzte möglich)
zurück
back retour
Letztes
Update dieses Teils +++ last
update +++ dernière
mise à jour: 08.08.2009