Erwachsenenbehandlung,
horizontaler Überbiss +++ Adult
treatment of horizontal overbite +++
Traitement de classe II (horizontale)
chez l´adulte
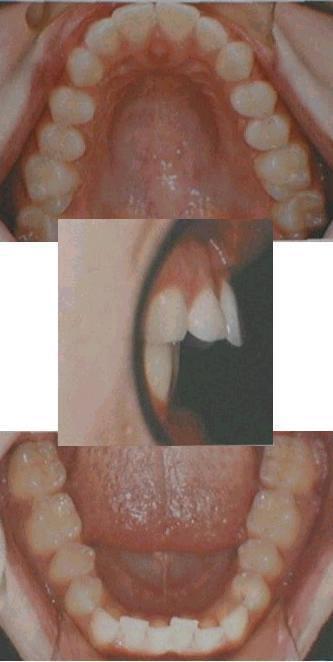
Die 19-jährige Patientin
in diesem Beispiel kam wegen ihres horizontalen Überbisses zur
Behandlung, der den Lippenschluss und das Abbeißen erschwerte.
Ursache war eine trotz „ordentlicher“ Zahnreihe frontale
Enge des Oberkiefers, so dass dieser nicht korrekt mit dem frontal
normal breiten Unterkiefer zusammenpasste.
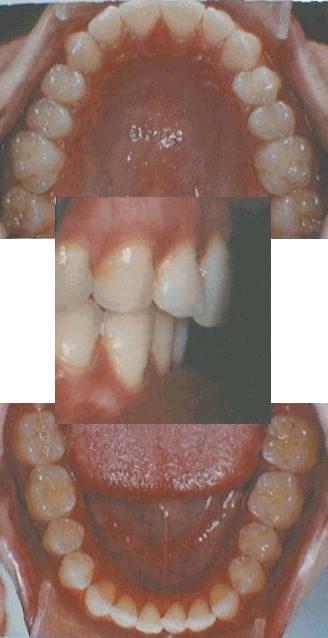
 In
einer 2-jährigen Behandlung mit dem gezeigten Plattenpaar mit
Vorschubschlaufen (Alternativlösung siehe Fallbeispiel
„Pro-Stab“), das 16/24h zu tragen war, wurde der
Oberkiefer durch frontale Weitung und sukzessives Rückschieben
aller seiner Zähne korrigiert. Die Weitung erfolgte nicht per
Fächerdehnschraube, sondern mit normaler „Dehnschraube“
und gezieltem Ausschleifen.
In
einer 2-jährigen Behandlung mit dem gezeigten Plattenpaar mit
Vorschubschlaufen (Alternativlösung siehe Fallbeispiel
„Pro-Stab“), das 16/24h zu tragen war, wurde der
Oberkiefer durch frontale Weitung und sukzessives Rückschieben
aller seiner Zähne korrigiert. Die Weitung erfolgte nicht per
Fächerdehnschraube, sondern mit normaler „Dehnschraube“
und gezieltem Ausschleifen.
Die Dreiecksklammern hatten nicht nur
Haltefunktion, sondern wurden, mit der hintersten beginnend, nach
hinten abgebogen zum Rückschub der entsprechenden Zähne.
Wobei sie, sobald eine hinreichend große Lücke geschaffen
war, im Hinblick auf mittigen Kraftansatz abgeändert wurden. Die
Front wurde anschließend mit dem Labialbogen zurückgezogen.
Im
Unterkiefer wurde die leicht beengte Front nach vorne korrigiert.
Es sei ausdrücklich
darauf hingewiesen, dass die solide Basis, die der Plattenkörper
darstellt, hier mit wenig Aufwand und wenig Patientenbelastung zwei
Maßnahmen ermöglicht, nämlich die Quer- und
die Längs-Platzbeschaffung (Distalisierung /
Mesialisierung), welche in der festsitzenden Technik belastende
Zusatzteile erfordern: Quer-Platzgewinn mit Quad-Helix (in der
üblichen Form eine Fehlkonstruktion, die die Zungenfunktion beim
Kauen massiv stört) oder im größeren Ausmaß mit
der riskanten Gaumennahtsprengung (auch fächerförmig),
Distalisierung gegen eine extraorale Verankerung (Headgear) oder
gegen eine Verankerung am Gaumen: Pendel-Platte, Distal-Jet, oder
neuerdings sogar invasiv als implantierte „Gaumenschraube“!
Kleiner, aber ebenso invasiv sind modische, zwischen die Zahnwurzeln
geschraubte Mini-Implantate, die niedliche Bezeichnungen wie z.B.
„Pin-Verankerung“ tragen. Welcher Patient denkt dabei an
Knochen-Piercing?
Eine allmähliche
Verbreiterung des Oberkiefers, nicht jedoch des Unterkiefers ist bei
Erwachsenen noch bis zu 4 mm möglich. Eine vorher gute seitliche
Verzahnung kann sich dadurch allerdings verschlechtern. Im
ausgewachsenen Unterkiefer ist Platzbeschaffung möglich durch
Schmalerschleifen und / oder durch Zurückschieben
(Distalisieren, siehe dazu
auch die Fallbeispiele Parallelverschiebung und Crozat),
oder schlimmstenfalls durch Ziehen des beengtesten Scheidezahnes. Zum
Ordnen der Zähne in die Lücke hinein kann mit aktiven
Platten ähnlich wie im Fallbeispiel „Mittenkorrektur“
verfahren werden. Mit Invisalign® sind solche Behandlungen auch
beschrieben.
 Allerdings
ist die Erwachsenenbehandlung mit Platten nicht so trivial, wie
es in der Kürze hier erscheinen mag! Zwar sind die Risiken und
Belastungen für die Patienten geringer als bei den für
Erwachsene üblichen festen Zahnspangen, insbesondere in
vorgeschädigten Fällen, aber für erfolgreiches
Behandeln sind auch hier Feinheiten zu beachten. Fachliteratur
konsultieren!
Allerdings
ist die Erwachsenenbehandlung mit Platten nicht so trivial, wie
es in der Kürze hier erscheinen mag! Zwar sind die Risiken und
Belastungen für die Patienten geringer als bei den für
Erwachsene üblichen festen Zahnspangen, insbesondere in
vorgeschädigten Fällen, aber für erfolgreiches
Behandeln sind auch hier Feinheiten zu beachten. Fachliteratur
konsultieren!
The
19-year old lady in this example came for treatment because of her
overbite, which impeded lip closure and biting off. The reason for
this overbite was that the upper jaw was frontally narrow, in spite
of its proper teeth alignment, and was therefore not matching well
with the lower jaw.
Treatment
took 2 years with the shown pair of bite-shift plate appliances, that
was to be worn 16/24h. The two thick wire arcs at the inside of the
upper plate are directed downward to shift the lower plate forward
(find another technical solution in case example „Pro-Stab..“).
The upper jaw was widened only frontally by acting the expansion
screw and grinding off plastic from the backward regions at the same
time. Alternatively, fan expansion screws are available for this
task.
Simultaneously, the many triangular clasps served not just
for holding the plate here, but were bent backwards one after the
other, beginning with the lastmost in the row. By this, the teeth
were shifted backwards one after the other. It is important there to
alter the clasps for a more central transmission of force, as soon as
the created gap allows for this. Subsequently, the front teeth were
retracted by tightening the labial bow.
In the
lower jaw, the slightly crowded front was shifted forward for space
gain.
It
is emphasized here that the rigid plastic body of the plate
allows the uncomplicated and simultaneous performance of two
frequent orthodontic tasks, namely the widening (expansion) of
the jaw and the sagittal movement of teeth (distalization /
mesialization). In treatment with fixed appliances, these tasks
would require additional burdens for the patient, like quad helices,
which disturb the tongue severely during chewing, or even splitting
of the palatal suture for widening, and headgears or fixed small
plates (pendelum, distal jet) for distalization / mesialization, or
nowadays even more profitable implants (micro screw, spiderscrew),
which expose the patient to the risk of severe inflammations!
For
children and teenagers, growth facilitates to do these tasks with
removables. For adults, a slow widening of the upper, but not the
lower jaw of up to 4 mm can still be achieved by this. However, this
can deteriorate the matching of the side teeth. Space in the
fully-grown lower jaw can be provided by slicing the teeth and / or
distalization (see also in the case examples Parallel
shift and Crozat), or in worst case by extraction of the most
crowded incisor. Subsequent ordering of the teeth can be done with
plate appliances similarly as in
the case example „Mid-line correction“, and has also been
described with Invisalign®.
 Note
well that adult treatment with removable appliances is not as trivial
as it may appear in this short outline here! The risks and burdens
for the patient are lower than for the commonly used fixed
appliances, in particular if already damages exist, but details have
to be considered for successful treatment. Adhere to professional
instructions for this.
Note
well that adult treatment with removable appliances is not as trivial
as it may appear in this short outline here! The risks and burdens
for the patient are lower than for the commonly used fixed
appliances, in particular if already damages exist, but details have
to be considered for successful treatment. Adhere to professional
instructions for this.
En cet
exemple, la cliente âgée de 19 ans venait pour
correction de son décalage horizontale, qui compliquait la
fermeture des lèvres et la fonction découpante des
incisives. Malgré des dents bien alignées, la
maxillaire antérieure était étroite, et par cela
ne s´adaptait pas bien à la mandibule.
La
correction a pris 2 années avec une seule paire des
plaques-propulseurs à porter 16/24h. Les éléments
propulseurs se trouvent ici au milieu de la plaque supérieure
(pour une autre solution technique, voir l´exemple de cas
„Pro-Stab“). En même temps, une expansion seulement
antérieure de la maxillaire est obtenu avec l´écarteur
simple et le rodage de la partie postérieure de la plaque.
Autre solution technique, qui pourrait être plus facile à
manier, sérait un écarteur en éventail.
Aussi
en même temps, les crochets triangulaires servaient pas
seulement comme crochets, mais étaient pliés en arrière
l´un après l´autre, pour pousser une dent apès
l´autre en arrière. Pour une bonne direction de la
force, il faut les modifiér aussitôt qu´ils
peuvent s´insérer entre les dents. Ensuite, les dents
frontales étaient poussées en arrière en serrant
le ressort frontal.
À la mandibule, les incisives un peu
étroites étaient alignées par poussée an
avant.
Il
faut souligner que le corps rigide et étendu de la plaque
permet d´accomplir facilement deux tâches qui sont
fréquentes dans l´orthopedie dento-faciale. L´expansion
et la distalisation (gain de l´espace en arrière)
sont possibles sans ces peines qui infligent les additifs des
techniques fixes au patient, soit pour l´expansion les quad
helix mal construits, qui dérangent la langue fortement, ou
même la disjonction palatinale, ou soit pour la
distalisation ou pour la mésialisation les forces
extra-orales, ou les plaquettes fixes, ou même des implants
orthodontiques (mini vis, vis cortical). Cet ancrage implantaire met
le patient en danger des graves imflammations.
Une
expansion lente de la maxillaire, mais pas de la mandibule est
toujours possible jusqu´au 4 mm chez l´adulte. Mais si
les dents des deux mâchoires s´étaient bien
adaptées auparavant, ça peut être dégradé.
Gain de l´espace à la mandibule adulte est possible par
minime rodage des dents et/ou par distalisation
(voir aussi les exemples de cas
Mouvements latéraux et Crozat), ou en cas pire par
l´extraction de la incisive qui est la plus coincée.
Pour aligner les dents ensuite, une plaque similaire à celle
dans l´exemple „Correction
de la ligne médiane“ peut être utile, et aussi des
traitements pareils avec Invisalign® sont connus.
Mais
tenez compte que le traitement des adultes avec les plaques amovibles
n´est pas si facile comme il semble peut-être dans ce
petit exposé. Les risques et contraintes qui porte le patient
sont certes moins comparé aux techniques fixes, en particulier
en dentition dégradée, mais il faut faire attention aux
détails pour avoir succès. Suivez des instructions
professionelles.
Quelle:
J. A. Lisson, „Behandlung erwachsener Patienten mit
Plattenapparaturen“, Kieferorthop 15 (2001) 313-22.
zurück
back retour
Letztes Update dieses Teils +++
last update +++ dernière
mise à jour: 04.01.2007